

Progression of chronic lymphocytic leukemia (CLL) on venetoclax (VEN) and BTK inhibitors (BTKi) is associated with acquired genomic variants in BCL2/MCL1/BCL2L1 and BTK/PLCG2, respectively, in some patients. We aimed to assess the clonal structure and evolution of resistance in patients (pts) with progressive disease treated with single agent VEN or BTKi (or both as sequential monotherapies) using next generation sequencing (NGS) and single cell sequencing.
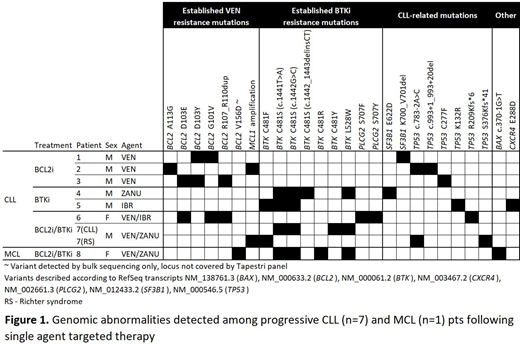
Seven pts with CLL and 1 with mantle cell lymphoma (MCL) with disease progression on VEN, ibrutinib (IBR) or zanubrutinib (ZANU) were identified from patients treated at our institutions. Pts were selected on the basis of multiple known resistance mechanisms from previous analysis of mutations (muts) and copy number changes detected using clinical bulk NGS targeting genes of interest including BCL2, MCL1, BCL2L1, BAX, BAK1, BTK, PLCG2, CXCR4, as well as TP53 and SF3B1. Of the 8 pts selected for single cell analysis, all had disease that was relapsed/refractory to chemotherapy prior to receiving either VEN (3 pts), BTKi (2 pts) or sequential VEN-BTKi (3 pts).
6,520-16,378 individual cells from 9 samples (8 pts) were analyzed (total 103,388 cells) using a custom panel targeting pt-specific muts on the Tapestri platform (Mission Bio). A summary of genomic abnormalities detected across the cohort is presented in Figure 1.
We first evaluated the relationship between genomic resistance mechanisms within the context of single agent (VEN or BTKi) as well as sequential VEN-BTKi treatment. In CLL pts treated with a single agent, all BCL2 muts in VEN pts and BTK muts in IBR or ZANU pts were identified in different subclones consistent with an oligoclonal pattern of disease progression with independent clonal acquisition of resistance mechanisms. Both pts who received ZANU (either as a single agent or sequentially) harbored the BTK L528W mut (previously described as enriched in ZANU progressors; Handunnetti ASH 2019) in independent clones from BTK C481 muts. In pts who received sequential VEN-BTKi treatment, clones were observed that harbored established or novel dual genomic resistance mechanisms within the same cell (BTK mut/MCL1 amp in CLL, BTK/BAX muts in MCL). However, this was not observed in all clones or for all pts, suggesting the presence of further undetected resistance mechanisms (genetic or other).
Given the unique ability of single cell sequencing to resolve mut context within a clonal hierarchy, we next assessed this phenomenon within our cohort utilizing other muts known to be present in these tumors. Analysis of TP53 muts exemplified the diversity of clonal patterns observed, with resistance muts being detected subclonally to parental TP53 muts in some pts and independently of TP53 muts in others. In addition, further evolution of resistant clones was observed through the development of TP53 muts within clones harboring acquired resistance muts, consistent with continued clonal evolution within the resistant disease compartment. In one pt, post-resistance clonal evolution was identified through the clonal acquisition of a CXCR4 mut within a BTK mutated population.
Finally, to understand the contribution of BTK zygosity and gender to BTKi resistance (given its location on the X-chromosome), we performed single cell analysis on a disease specimen from a female pt with progressive MCL harboring multiple BTK mutations following treatment with sequential VEN-BTKi. Analysis revealed four clonally independent heterozygous BTK muts inferring the sufficiency of a single mutant allele to drive resistance in this context. Interestingly, this pt also harbored a BCL2 mut and a BAX mut, the latter co-occurring with a BTK mut (BCL2 not assessable). This pt therefore represents the first description of BCL2 or BAX muts occurring in a pt with progressive MCL on VEN and the first of a BTK L528W mut in MCL progressing on ZANU.
In summary, these data highlight the significant clonal complexity of CLL progression on VEN and BTKi. Our data show that disease progression in this context is consistently oligoclonal with separate clones harboring distinct identifiable resistance mechanisms. These data have pt-specific implications for the potential utility of cycling back to previously efficacious targeted therapies as well as providing a strong rationale for the early use of disease-appropriate combination targeted therapies.
Anderson:Walter and Eliza Hall Institute: Patents & Royalties: milestone and royalty payments related to venetoclax.. Handunnetti:AbbVie: Other: Travel expenses; Roche: Honoraria; Gilead: Honoraria. Yeh:Novartis: Honoraria; Gilead: Research Funding. Tam:BeiGene: Honoraria; Janssen: Honoraria, Research Funding; AbbVie: Honoraria, Research Funding. Seymour:Morphosys: Consultancy, Honoraria; Mei Pharma: Consultancy, Honoraria; Gilead: Consultancy; AstraZeneca: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Janssen: Consultancy, Honoraria, Research Funding; F. Hoffmann-La Roche: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Celgene: Consultancy, Honoraria, Research Funding; AbbVie: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Nurix: Honoraria. Roberts:Janssen: Research Funding; Servier: Research Funding; AbbVie: Research Funding; Genentech: Patents & Royalties: for venetoclax to one of my employers (Walter & Eliza Hall Institute); I receive a share of these royalties. Blombery:Amgen: Consultancy; Novartis: Consultancy; Invivoscribe: Honoraria; Janssen: Honoraria.

